Select a link
below, or just start reading from here for my experience from
2013 onwards (warning - it's a long read!).
Note that what I have written relates to the time of writing.
I started writing this blog shortly after my Cryotherapy
procedure in 2014.
Brief
introductory summary:
Autumn 2013: PSA 6.2. (My age then: 60 years). Cryotherapy spring
2014. PSA then 3.1
Autumn 2018: PSA 5.2. HIFU spring 2019.
Then in 2020: radical prostatectomy.
Recommended
route for all men aged 50 or over:
1. Have a PSA blood test at least once
a year.
2. If the value is above 4, then repeat every 6 months.
3 If, over 1 to 2 years, the value shows a steady increase, then:
4. Ask for a Prostate MRI scan.
Nearly 10
years after I started this blog, the BBC News has caught up. See
these two videos from 2023:
What
they fail to mention in
the video above, is the value of monitoring a
trend in PSA levels.
See my blog below for how this was successfully done in my case.
However,
it is true that, had I
had an MIR scan around 3 years earlier (than 2013) say, the year
2010,
then my tumour would have been discovered at an earlier stage. But my feeling is it's doubtful that this
would have been of much significance,
since I would have likely had the same biopsy and treatments that
I actually had.
I will admit that
this blog may appear a bit disjointed. However, I
have built it up over several years, from the
time I was originally diagnosed with prostate
cancer in September 2013.
To begin with, it was a shock to hear my
diagnosis, and hence my earlier notes may have
been one way of “venting” my feelings
during that time.
However, without completely re-writing the whole
blog, I still
hope it will give some helpful details I have
discovered during my experience.
Please note: this blog
includes a summary of what you can find elsewhere
on the web.
My purpose of this blog is to share my personal
experience of my Prostate Cancer investigation,
diagnosis and treatement from
a patients point of view.
It also contains some personal medical
information about myself.
I am happy to share this, because my desire is to
try to raiseawareness
of the improved diagnostic
and treatment procedures
for early stage prostate
cancer. This I hope to do through describing my
personal experience.
Note that the MRI I had and
Template Biopsy are available on the NHS (see
discussions later). Most of my treatments were carried out on
the NHS.
Obviously, I am
not a qualified medical practitioner.
I am a patient, describing my
experiences, and commenting on my
observations. I think the legal term is:
I'm "acting entirely in a personal
capacity" (!) Always
consult with a qualified medical
practitioner before making decisions
regarding your own personal treatment.
I would advise every
man aged 50 or over to have an annual PSA blood
test.
This can be arranged through your GP. And, yes:
if you think it is difficult getting to see your
GP - Persevere!
It is much less hassle than having Prostate
Cancer develop undetected, until it is too late!
Around 37,000 men in the
UK are diagnosed with prostate cancer each year
It is a medical
statistic that black men are twice as likely to
get prostate cancer than white men.
I am 61 years old (as of
April 2014), and had a significant prostate
cancer tumour, but only knew about it originally
thanks to having 6-monthly PSA blood tests. I had
no other symptoms.
Below are my PSA
readings over the past 6 years (pre-procedure).
See also comment
and latest
results
2009
2011
Mar
2012
Jan
2013
June
2013
Jan
2014
2.61
3.94
4.19
4.93
6.2
5.8
To compare
these PSA readings with those up to 2018, click HERE
In 2013, my
cancer tumour was then definitely confirmed using
the technique in the video below (MRI September
then TPM Biopsy October) (and, no: I'm not the
actual patient in the video, but I would have
looked much the same!) Please note
that this Template Biopsy is
now available on the NHS
at UCLH and other NHS hospitals
Warning: contatins some
graphic content
I had the above TPM Biopsy in
October 2013, under a very short general anaesthetic. As
Emberton explains in the video, it's important that the
patient is very still.
It was probably lots more comfortable than having it
under a regional (local) anaesthetic. My recovery was
about 3 hours, so not much different to recovering from
strong sedation.
For those of you interested in
my actual biopsy samples taken, click
here for the histopathology
report sheets.
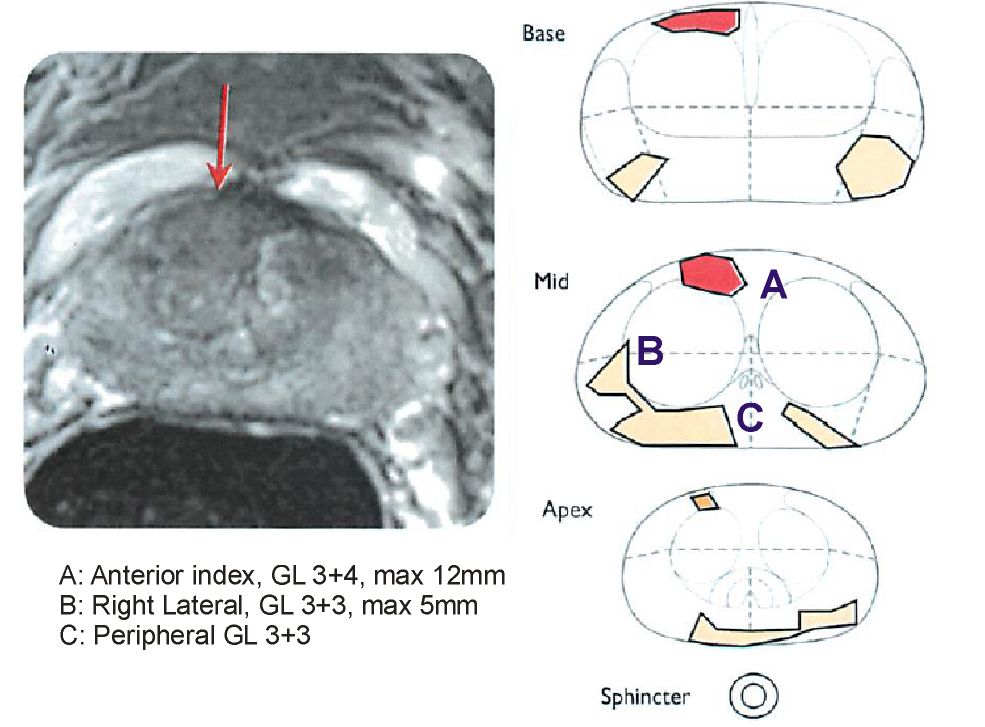
Below is my
diagnostic MRI scan (September 2013), showing an
"80% 1cc likely tumour" (Red areas on
drawings)
My TPM Biopsy (as
discussed in the video above) then confirmed it
was localised prostate cancer (12mm Gleason 3+4).
For those of you
interested in my actual biopsy samples taken, click
here
for the histopathology report sheets.
The treatment technique
I initially chose was Focal Hifu.
This appears to be an excellent treatment, but
see later.
IMPORTANT!! My cancer WAS NOT detectable on:
1. Digital (finger) rectal examination
2. Ultrasound scan (rectal)
3. Emberton said that the more common TRUS biopsy
would most likely have not detected my anterior
tumour. See first video
regarding this.
Hence it's essential to
start having an ANNUAL PSA blood test once you
reach age 50. I anticipate I'll do that for the
rest of my life, and so should every man. A blood
test is SO simple!
If you want to skip
straight to my results after my surgery, please click
here
The video below explains
HIFU, and also mentions Nano Knife:
If you want to
know more details of what happens in the above
video, the Patient Informatioin Sheet below
includes details of HIFU. Please note that this
also includes extra after-test details, which
only apply if it's done as a trial at UCLH. I was
originally going to have it
"off-trial", hence these extra
after-tests wouldn't have applied.
Originally Emberton was going to give me Nano Knife privately at
Princess Grace Hospital. However, since my insurance didn't cover
that hospital, I transferred to UCLH for my cancer treatment.
At that time, Nano Knife was being trialled at UCLH on the NHS,
but I didn't qualify since I also had other residual prostate
cancer, see my diagnostic MRI scan above.
Every patient in England has freedom of choice to selelct their
preferred hospital
See the referral
contact details below.
I wanted to continue treatment under Emberton.
UCLH was not my local hospital, so I specifically requested to be
referred to it.
I originally said
I'd have HIFU at UCLH, but on reflection, considering the
location of my tumour, I decided that Cryotherapy would be
better, since it wouldn't have also ablated my prostate near the
rectum.
WHAT
HAPPENS DURING CRYOTHERAPY?
Watch this video made by Galil, the designers of the
machine used on me.
The
above video appears to show whole
gland therapy, rather than the focal
therapy I had. Emberton says I should end up with only
about 5cc of my prostate ablated, which sounds
"pretty good", should leave around 23cc of my
28cc prostate! Unless, I can come up with a more
precise therapy!
For
the UCLH patient info for Cryotherapy, click here
I
had the cryo surgery on April 22nd 2014. To read how it
went, - click here
A further brief
discussion of the advantages of these diagnostic
and therapy methods was aired on a BBC Inside
Health radio program in January 2014. See the
video below:
Nano Knife
appears to offer considerable advantages over
many other forms of focal therapy. It may cause
less localised good-tissue damage, plus offer a
quicker recovery time. Also, the precision with
which it can be used may make it ideal for
destroying very small tumours.
The
following notes were made early on in the year
2014, during my investigations of my options for
my prostate cancer treatment. [this note added
24th Dec 2014]
[March
2014]: UCLH are undertaking a new
treatment, called IRREVERSIBLE
ELECTROPORATION (‘NANOKNIFE’).
This may offer slightly more localised
treatment, but is only being offered
to patients with no significant cancer
outside of the anterior (away from the
rectum) side of the prostate. I did
not qualify for this.
To see
the Webcast where Prof Emberton answers
viewers questions, click
here.
NanoKnife is mentioned in the video at
the 19 minutes position, when he replies
to my email.
[Tuesday
22nd April 2014] Cryo went well yesterday . Had
typical post anaesthetic vomiting reaction.
It was
delayed for about 3.5 hours. The reason enables
an insight into the issues that must regularly
face the hospitals.
I had even got as far as lying on the trolley in
the anaesthetic room. Had a cannula inserted.
Then, possibly just in time, before
they started the
anasthetic, I was told I’d have to be
wheeled out and wait about 45 minutes.
The ultrasound monitoring machine was still being
used in another
theatre. They needed this machine for me.
I could understand the reason – it was being
used for a TPM biopsy (see video for chat about that).
However, after about 90 minutes waiting, I
discovered, by asking, that another patient had
now gone into “my” theatre, who
presumably didn't need that machine for their
operation (which may have been, therefore, a more
serious operation than mine).
Whilst it was
frustrating, having had myself the TPM biopsy
last year, and knowing whom the other
surgeon was
who was using it at UCLH, it made it easier to
understand and tolerate.
I was discharged from UCLH following morning.
Surgeon was also thinking of
zapping the right lateral (see MRI pic), but I said only do
anterior index.
No pain from cryo – instead, just discomfort
now wearing 7-day catheter, to be removed 28th
April.
Won’t know initial results until after MRI on
10th May.
Other side effects- I assume it’ll take
several months before the extent of the various
possible permanent side-effects can be
determined. Surgeon said possibly only 20%
chance dry climax.
Had visit from district nurse 2 days after
surgery, who helped with a few catheter issues. Surgeon emailed me a few days after
surgery, said:
"Hi Andrew - yes spoke with you in
recovery!" [Although I don't remember it -
Amnesia after general].
"Procedure went very well and I'm very happy
with the way it went.
"Yes we use a local anaesthetic [on
perineum] at the end of the procedure.
I agree the catheter causes more discomfort than
the procedure but hopefully will be out soon.
MRI in 2 weeks will give us a good idea about
treatment but I'm confident the [index] lesion
was well treated."
Hoping
to return to work on 6th May. Surgeon suggests taking it easy: no
cycling for 6 weeks (pity - there's a tube strike
next week!), and "no heavy lifting or
straining" for 4 weeks. Today [1st May] I
bought a box of printer paper. So, asked the PC
World assistant to carry to my car. Then, brought
it up to my flat max. 2 reams at a time.
[22nd May 2014]: Very
pleased to report that my continence and erectile
and ejaculatory functions all appear to be
largely unaffected.
[29th June 2014]: Ejaculate
does seem to have diminished over the past month.
However, it's difficult to assess it, since it
was never that consistent before
my surgery.
[28th April 2014]
6 days wearing a urethral catheter –
uncomfortable, and often painful! The
paracetamols they gave me were a great help,
although they were really intended for any otherpost-surgical pain, which I actually
didn't have. So, a great relief to have the
catheter removed today!
Yesterday felt like I had a fever (probably my
body trying to reject the catheter, but
controlled by the antibiotics). (see also surgeon's
comment
on the catheter above)
Catheter removed today – far less painful
than I thought . The clinic nurses told me to
"take a deep breath" twice during the
removal. It sounded like I was giving birth! LOL!
Very pleased with initial urine control test
results – NO leakage! And 100ml retention
was considered ok by nurses, and I think it may
improve with time. Pee-ing is quite uncomfortable
at the moment, but I know from experience [as
after my TPM biopsies] that that will disappear
within a few weeks.
And again, a great service from all the staff and
nurses at UCLH!
[4th
May] Having second thoughts: it may have been my
general reaction to the surgery, rather than the
catheter alone. Guess maybe part of healing
process? Don't feel to terrific today, either.
Think my walk of 2.5 miles to Church this morning
for exercise may have been a bit ambitious!
Why did I choose Emberton as
a urologist, rather than a urologist at my local
Croydon Hospital?
[3rd May 2014]
Simple answer is, from Google
Retrospetcively, I can see it was an answer to
prayer. He is one of the top urologists, and
specialises in minimally invasive solutions for
prostate cancer.
I have private medical insurance because my
company has a group scheme. So, I decided to find
a private urologist close to my City office, so
as to minimise time off work for consultations.
Google flagged Emberton up, since he runs a
private clinic in addition to the work he does at
UCLH, (see “useful links” section). Because of
his desire to have much of his work in the public
domain, it was easy to see the techniques he was
using, before
my first consultation. Simply googling his name
brings up much about his work on the web,
including youtube.
I’m thankful to God that I found him,
because before then, all I knew about was the
radical treatments: prostatectomy and radiation,
neither of which are necessary for my condition, unless
the patient has a personal desire to have the
whole prostate removed. Also, I'd never heard
of the TPM biopsy, only the
TRUS one. See the
first video
on this page, for a discussion about this.
So, why am I now being treated and monitored by
his team at UCLH, which is an NHS hospital?
Well, my company medical insurance doesn’t
fully cover Princess Grace hospital, which he
uses for the treatments. I was happy to pay
£1,000 towards the TPM biopsies, but Nano Knife
would have cost me around £4,500, plus more if I
needed further surgery because of complications.
Hence, I’m now over to UCLH. It’s a
really great hospital. It has a more relaxed
atmosphere than what I’ve experienced at
some other NHS hospitals. And, the surgical
treatment is identical to what you get in the private
hospital. In fact, most of the surgeons operate
in both
hospitals! The obvious disadvantage is longer
waiting time at UCLH. However, to me, that had
two advantages:
1. It allowed me more time to study my condition,
and consider the various options. True, my final
cryo treatment choice is very similar to what he
would have done privately within about 10 days.
But, for me, there’s a great advantage in
understanding more about my condition.
2. It means that I can now pass on my experience
here, as an NHS patient. That’s what the
majority of you who read this would come in as,
should you need to be referred to the UCLH team.
Emberton said that,
ideally, I should have gone to him for the MRI earlier,
when my PSA readings were about 4.
PSA readings can
vary, it seems, by as much as nearly 1, in my
case. One of my relatives PSA read 4.5, then 6
months later, about 2.5! (It seems unlikely that
he has cancer).
Hence, I get the impression that "4.19"
could really be "3.8" or
"4.6". However, it is the steady
increase (from about 2 in 2009 to about 6 now)
that is the more meaningful indicator.
PSA readings can be high merely for an infection,
not always cancer.
In my
case, and for general
prostate cancer screening, the important thing
seems to be observing the trend
over at least 3 or 4 readings, spaced about 6
months apart. This is how my (excellent) GP
advised us to monitor my PSA.
Personally, I would
have thought it better to give figures rounded
up/down to the nearest whole number, without
bothering with the decimal place.
Prostate cancer is slow to
develop: you won't suddenly get it "breaking
out" and killing you in 6 months! It's easy
to think it
might, because, sadly, some other cancers can
do that. But not prostate.
Please note
that it is very easy
to have annual or 6-monthly PSA tests. Mine were
taken at my very excellent NHS GP surgery (but
obviously then sent off to be analysed by the
path. lab. at the local hospital). I had them
done at the same time as my cholesterol tests
(same single blood sample taken, but 2 parameters
checked for by the path lab).
You have every
right, even under the NHS,
to be told your medical test results. My GP
happily phoned me up each time, to discuss them.
It will be
interesting to see by how much my PSA reading has
dropped since my surgery. I'll publish the figure
when I've had my next test (I now know this will
be in November 2014).
[6 June 2014]: As
my GP has just reminded me, PSA can also be an unreliable
marker.
It could equally well signal an enlarged
prostate, and not
necessarily cancer.
However, I still
feel that's erring on the safe
side.
All it takes is an
MRI to verify if prostate cancer is present.
That's a test, not treatment.
So, it can't be classified as over-treatment.
In my
case, I eventually had
cryotherapy only becase
the initial MRI showed an 80% likely tumour.
Hence, over-treatment did not
occurr: I needed
the treatment.
Found
this page helpful? Want to share your
experience with me?
My
MRI scan after my surgery
[10th
May 2014, Saturday]: Had my post-surgery MRI scan
this Saturday morning in the NHS UCLH hospital.
Was pleased with their efficiency: no waiting
around.
Also,
the radiologists were happy about my taking the
one Temazepam 10mg (as a mild sedative) about 20
minutes prior to the scan; they agreed that about
1 hour "hanging around" after the scan
should render me ok to travel on public
transport.
Well,
did that help?
Answer: yes! Certainly didn't feel claustrophobic
like I did last year (for the results of that
MRI, see above.
So,
what will be done with the results? Well, my
consultant will receive the report, and I expect
a consultation to discuss it soon.
You
notice I had the radiologist report for my first MRI. Well, I asked the
radiologist if I could similarly have that, plus
the full CD of all images, after my scan today. I
was told to contact them during the next working
week. There would be a charge to pay.
[13
May] Picked up copy of CD of MRI images
today-there was no charge, since I got them
within 40 days. Was told that the radiologists
don't also give a detailed annotated report as
for my first MRI. I now realise why - this second
MRI merely looks for the ablated
area, so will not report on remaining cancer, I
presume.
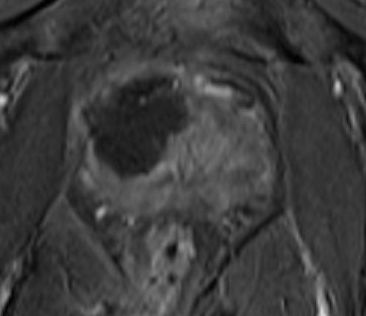
The
image below shows the cryo ablated (destroyed)
area-
the dark area.
The surgeon says "it looks very
good", so I presume that means he ablated an
ideal area.
(Remember:
"left" in the image is the right
hand side of my body)
I must say, the area ablated looks much
larger than the red area marked on my first MRI. However, the surgeondid say
that he would target an area a little larger than
that, to be sure all the
index lesion was killed off, plus I guess the
precision of the cryo comes into play.
If,
like me, you ask for and get your own
CD copy of your MRI images
[which you have every right to do, free, even on
the NHS], you may need to download
a MicroDicom viewer to be
able to view the pictures. This is the one I used
for Windows: Click here for the viewer it's free for 30 days
(trial license). This "RadiAnt" version
is incredibly good! it handles both my private
pre-op images and my
post-op NHS ones, unlike the first viewer I
downloaded and tried. You can even measure
portions of the image, in
linear and square quantities! There are even
better viewers for Apple Mac. Very limited choice
for Android, don't know about iphone.
[15th
May]: follow-up appointment to discuss things
with the surgeon arranged for 28th May. PSA
blood test yet to be arranged, but been told will
be around 2-3 months time (update
- see below). Need to note
down questions to ask him.
[13
June 2014]: I'd be interested to know what tissue
has replaced the
tumour and good tissue that was ablated. Some
months ago, "scar tissue" was mentioned
by another
surgeon
whom I talked to at UCLH.
Latest updates follow here -
my attempt to keep a log of tests, procedures and
results that are continuing
Most recent results are listed first.
Update 27th July 2025
Latest reading: My PSA reading in November 2024:
less than 0.100
ug/L
which, as before, means it is likely undetectable. I
would prefer it taken to a better
resolution like before, but they won't.
Continence: still the same as before. Only occasional
leakage, so those self-fashioned pads mentined below are
adequate.
Update
4th March 2024 (yes, I now have
annual check taken by my GP nurse or local hospital
bloods clinic - was GP nurse this time. I have had it
more frequently before, but this time my GP checked my
UCLH discharge instructions, which says it should be
annual) My PSA reading: less than < 0.014
ug/L which, as before, means it is undetectable.
Erections:
Standing or kneeling up, without Sildenifil 50mg, with
stimulation, I can get reasonably firm erections. Often,
but not always, by taking one Sildenifil 50mg about one
hour before, I can also get an erection lying down. As
before, not being married, can't tell if it's adequate
for intercourse.
Update
27th February 2023 My PSA reading: less than 0.014,
"which is undetectable", says my GP.
Update
24 January 2023: Continence: still
sometimes leak a very small amount if I cough or strain a
bit, but easily absorbed by one of my
"home-made" pads (see earlier).
Update
September 2022: It does not appear
that I will ever return to my pre-surgical continence. I
will always have a weakness, although (see below), I can
often manage a whole day without leakage.
Update
9 August 2022: PSA level less than
0.01, hence classified as undetectable.
So my next PSA test is due in August 2023, although, like
before, I may have it earlier if it's taken at the same
time as any other bloods before then.
May
2022 Continence: Very much improved -
now, it's been 2 years 2 months since my surgery.
Hardly ever leak, except sometimes (not always) when
straining to pass wind, or having just finished a cycle
ride and changing from firm-fitting cycle briefs to
normal underwear. The hospital told me that's because
I've been sitting on my perineum.
I can normally manage a whole day without one of my small
pads,
however I've found one advantage in using them: I can
wear the same underwear for 2 or 3 days, since the pad
absorbs moisture and odours.
Erections:
with physical stimulation, I can now get reasonable
erections, to the extent that Sildenifil 50mg makes no
improvement - I don't appear to need them. Don't need the pump either. Not able to tell
if it's adequate for intercourse, though.
I don't, hower, get spontaneous
erections like I used to, but I do
sometimes get a slight spontaneous lenghening, althugh
it's not firm.
So, maybe there can
be hope this will improve further with time.
January
2022 Now "signed-off" from the
hospital back to my GP.
Latest PSA less than 0.01 (=undetectable)
If it rises above 0.l, then GP is to contact them.
Also if any issues I can email the clinic nurses any
time.
When
I asked why not GP contact them if PSA rises above a
lower level (say, 0.03), they said they'd not be able to
detect a reason at that low a level, i.e., an MRI
wouldn't show anything. Anyway, I no longer have a
porstate to perform an MRI on!
Leakage:
as far as I'm concerned, it plateaued about a year ago
[but see above]. Still only occasional leakage when
caughing, straining, which is not uncommon for men of my
age (nearly 69), even if they haven't had a prostate
operation.
Erections:
very good using 50mg Sildenifil together with
stimulation. Also can get a reasonable erection without,
sometimes.
4th
June 2021 My progress so far.
Had teleconsultation with Andrology Registrar regarding
my erectile disfunction.
I was able to report that Sildenafil 100mg gave me good
erections. Also reported the cyanopsia (blue tint to colours)
that I get in my vision for a few hours with the
Sildenafil. He said that's not a problem, so long as it
doesn't persist continually.
Still
only get erections by doing physical stimulation. Was
told that might never improve, due to having had only one
nerve spared (see below). He both nerves would have
needed to have been spared to make that a small
possibility.
But
he did emphasise the importance of getting erections
reguarly (not necessarily every day), to prevent penis
shortening.
And he mentioned something I'd not thought about - for
younger men, miltiple nightime spontaneous erections are
normal, which maintains penis length. This diminishes
with age, and has dissapeared altogether in my case.
He
said either use Sildenafil or the pump to obtain an
erection, for the above reasons. But it's likely, I
think, that using my constriction device (see below) may
be a third method; however, my personal thought is that
this merely maintains erections;
it doesn't of itself increase the blood flow, like
Sildenafil or the pump does.
He's
now discharged me back to my GP, saying I can always ask
to be re-referred back to him in the future, if the need
arises.
4th
March 2021 Teleconsultation with prostate
clinic nurse.
Was pleased to be able to report slight improvements all
round.
Very slight improvement in continence: still hardly need
to wear a pad.
Caughing can cause very slight leakage if I don't think
to do a squeeze beforehand, but even then only a small
amount, much like just after shaking after a pee.
Also after cycling; as I suspected, the hospital today
confirmed that would be because I've just been sitting
with my perineun on the saddle. Short-term effect on my
lower sphincer.
ED:
using pump has made a slight improvement (bear in mind
that I could already achieve a reasonable non-rigid
erection before having it, see notes earlier), but still
no firm erections without a constriction device.
Have now fashioned my own one, based on an item for sale
online, see below. Made using part of a drawstring from
an old pair of swim shorts, and a toggle!
Using this, and without the pump, I can achieve a fairly
firm erection. But no spontaneous erections; still need
to use physical stimulation. Obviously no ejaculation.
Orgasm and climax remains very good. (To reiterate: they
spared one of my nerves during surgery - "unilateral
nerve sparing")
General
comment from hospital is that I'm doing very well,
considering I also had HIFU in 2019.
Both continence and ED likely to further improve over
time.
14th
January 2021 So, how have I been getting on with
the pump?
First, I'll mention a few tips.
The lubricant
they supply: I figured it'd run out after around 20 uses.
Then I'd need to order it free (I'm over 60) on
prescription again.
So, as an alternative to the lubircant, I made up a
strong hand-soap/water solution. Whilst runnier than the
lubricant, it is sufficient to make a seal. They claim
other lubricants (like you can get online) will damage
the rubber rings etc. But I reckon that soapy water is
ok, since that's how they suggest you clean the pump
tube.
As they mention in the instructions, shaving pubic hair
around the base of your penis helps achieve a vacuum
seal. I use a "personal
grooming shaver" - there's loads out there to
choose from.
Has
it helped?
Well, in my case, over the months since my surgery in
February 2020, I've been trying to occasionally get an
erection. So, since I've likely already been
rehabilitating my penis, this pump hasn't made a lot of
difference. But I've not
been able to achieve as hard an erection without it
before, but I do need to use their tension device (ring)
to maintain that erectioin.
My overal opinion When used to get and maintain an
erection, it's not as comfortable as I'd hoped.
Maybe I'm still using too small (tight) a tension device
(see video). I get an unpleasant pinch feeling.
I've yet to try one of the larger tension devices that
came with the pump.
Since I don't have a wife, I can't comment if I get an
erection suitable for insertion/penetration. However,
from my experience when my late wife was alive, I think I
could manage insertion with a less hard erection - using
a looser, less effective tension device. But obviously,
this will depend on individual couples.
Possible
beneficial secondary effect:
Improved flow: This does
seem to have improved since using the pump! In fact, my
flow when voiding is better than it was before my
surgery!
Also, I think (difficult to tell: may be due to just
being more relaxed) it helps me to not get up so often in
the night. I was typically getting up for the bathroom
twice until about a month ago - now it's normally only
once a night.
Important observation I still do not
get a spontaneous erection. I can
"work-up" a reasonable, but not
"hard", erection, without the pump, but using
my improvised "rubber-band" ring. If I do this
just prior to using the pump, find I obviously get a hard
erection (in the pump) quicker.
It takes a lot longer
for me to "work up" an erection without the
pump, than it did before my surgery. I guess this is
because there's no spontaneous erection possible yet.
Will spontaneious erections ever return? From what I've read/heard, maybe in
a few years time.
But, I'll keep you posted!
27th November 2020 Andrology appointment at UCLH
Purpose: to try/learn how to use a penis pump.
Was
instructed and supervised by the clinician. Yes, really
on myself. Yes, he firmly locked the door and checked the
window blind beforehand!
Basically, it was how you see in the video below: If you don't see the video
below, then click here
Was
it effective? Very! Obtained a pretty firm erection,
which I've been unable to do even when using my own
improvised penis rings.
The
main purpose for me at present, is to rehabilitate
my penis, reather than only using it for getting/holding
an erectioin.
Did I
bring it home? No, it was his demo version. But he was
able to see what size rings I needed.
He
was effectively a clinician-representative for the
iMEDicare Ltd company. He gave me a list to give my GP of
all the relevant items, the idea is that my GP will then
write me an NHS prescription for it.
7th
November 2020
Urine leakage
Thankfully, I'm noticing a significant improvement, for
which I praise God.
Most days, I now do not wear a pad or any part of one
whilst indoors. I can squat without any leakage*, and
when caughing only occasionally a slight feeling of
leakage, but no significant soiling of underwear - not
much different to normal pre-surgery after-urination
dampness. I'd like to see if I leak at all in a pad next
ime I'm outdoors for a significant lenghth of time,
before I'm confident enough to not wear a pad then*.
This
is most
encouraging, and may indicate that, buy next summer, I'll
most likely not need pads at all, and will be back to
normal!
*1st
update 20th November: squatting and leakage: I do
get some leakage if I perform squeezy exercises whilst
squatting with my lower back against my sofa; kind-of
half sliding off. This only happens during the fast
squeezes. It's effectivey sqeezing and relaxing every
second, and the quick relaxes are probably close to
relaxing when pee-ing. Will discuss on Thursday 3rd
December during my hospital teleconsultation.
*2nd
update 20th November: I have managed to take short
outdoor walks without
any pad, and normally have not leaked.
Erections
By using my own improvised penis ring (two very small
rubber bands!), I almost get the erections I did before
my surgery. But no spontaneous erections yet (without
stimulation, and no "early morning boners").
Climax remians good.
27th
August 2020
Hospital telephone consultation Prostate clinic nurse Karen from
UCLH phoned.
I was able to report my improvements as below.
She reiterated that my PSA of 0.01 meant an effectively
undetectable level, which is very good.
My leakage - she said that I was doing very well,
particularly considering that I've had two lots of focal
therapy over the years, before my ultimate radical
prostatectomy.
She said that I should continue with squeezy exercises,
it should speed up my probable full restoring to not
needing pads. So I'll try to increase from my present 1 a
day.
I told her also of my recent ED results (see below), which she noted.
My
next UCLH appointment is 26th November, for a physical
consultation with the Andrology team to have a penis pump
demonstrated. The mind boggles!
25th
August 2020 Urine leakage: improved from a few
months ago; very little, some days none at all. Mostly if
I cough or squat then stand up.
Still doing one squeezy exercise per day, but I feel it
now makes no difference - I've plateaued to no further
improvement. From what I've heard, I may be completely
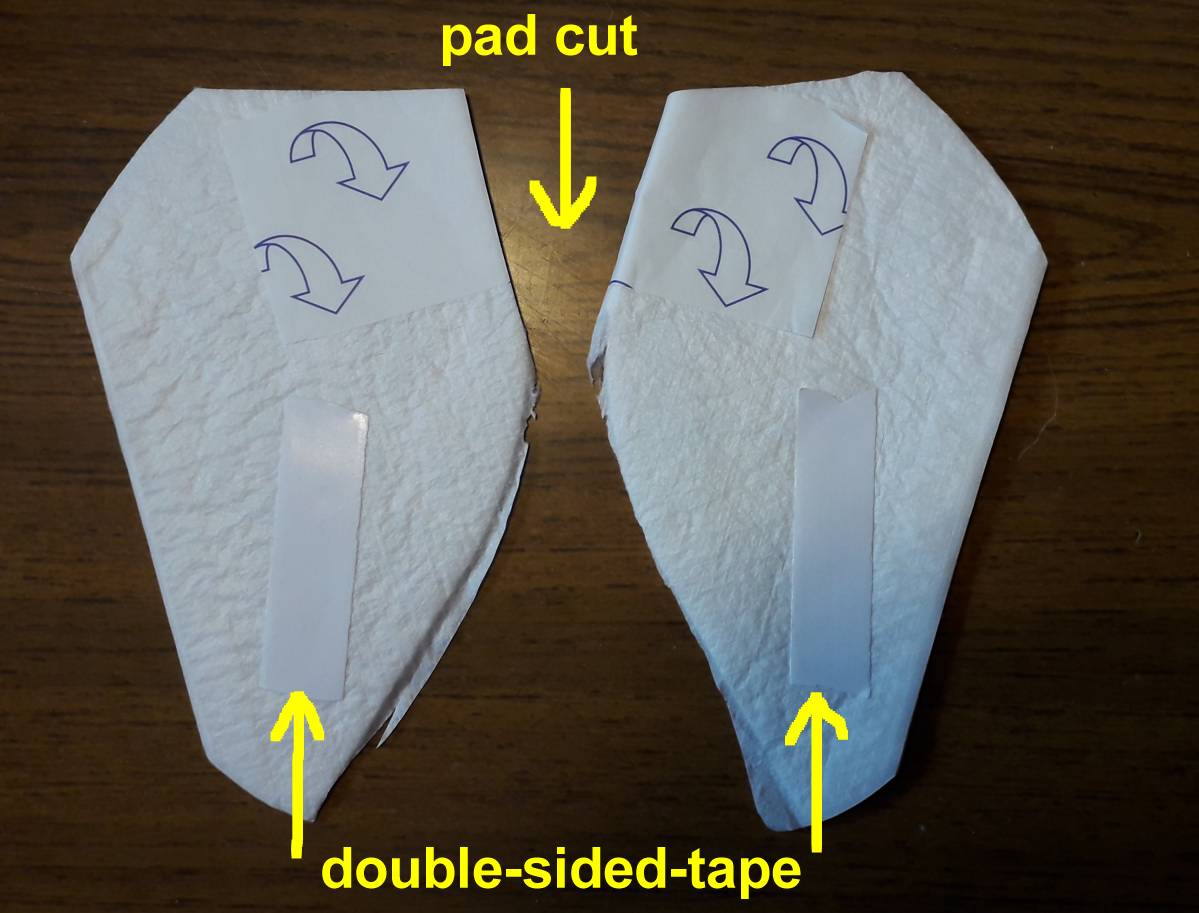
leak-free in about 1 year's time. Pads I'm using:: Boots
Staydry Men Shields For use around the home, and
occasional short expeditions outside, I cut each pad in
half, and add a bit of double-sided tape! But for a full
day or more away from home, I wear one whole pad. This is
for my own confidence; the half-pad would still probably
be adequate for me.
Update: have since much improved - see updates above in
2022.
21st August 2020 PSA blood test result from UCLH: PSA
= 0.01 (compare with 0.03 on 15th May)
UCLH intepret that as undetectable. So, praise God, no
indication of any residual prostate cancer!
21st
August 2020 ED results Picked up from the
chemist, Sildenafil, (sold under the brand name Viagra
among others) 50mg tablets. These were requested by UCLH
to my GP.
Supposed to improve erections.
Tried one: helped a little, but not a reasonably firm
erection until I used a small rubber band (as an impromtu
penis ring) at my penis base.
Climax seems to have reduced these days.
Don't have a wife, so can't comment re. "firm enough
erection for intercourse" etc, but my guess is that
I might have managed it
28th
May 2020 UCLH Follow-up consultation with
Prostate Cancer Nurse
A couple of extracts from her letters afterwards:
[To Professor
Ralph]:
"..........He has not noted any return of potency.
He wishes to be seen in your clinic and explore treatment
options that is available for him. He also would like to
be shown how to use the vacuum pump for penile
rehabilitation. I will be grateful if you can offer him
an appointment to be seen in your clinic.
[To
my GP]: "...advised to [perform] [squeezies] a maximum of 5 times/ day
instead. As performing a lot of repetitions may not help
build his pelvic floor muscles." I had stopped
altogether, since it didn't seem to be reducing my
'leaking' any further.
i'm planning on doing 3 per day.
23rd
May 2020 I've found I can manage with the normal pads.
Also, I use only half a pad, cutting it lenghways along
the fold, then adding my own double-sided tape on the
waterproof side. This may not work once I get more active
if/when I return to work; I may need a full pad.
Next
consultatioin (presumably by telephone again) with the
clinic nurse on 28th May. So, what's happend over the last few
months?
Well, my recovery at home has merged into my being
furlouged, because of the national lockdown.
To help my "mental health", I've found
something to do for the NHS. See what you think of my
efforts!
So what of my recovery? It's been an exceptional
experience!
I've seen the hand of God in this: my cystogram and
catheter removal was originally booked for more than 3
weeks after my surgery!
Not only did I not want the wear a catheter that long,
but the worsening Covid-19 situation was steadily
shutting down routine hospital procedures.
However, with the help of the excellent prostate nursing
team, contactable by email, that appointment was brought
forward to 12th March.
MY
PSA as of 15th May: 0.03 ug/L. As
far as I am concerned, that means not measureable!
31st
March 2020: Telephone consultation
with Dr Anthony Ta.
Histology report on my removed prostate: All good, praise
God! Cancer is well confined to prostate, not spread to
the capsule (thin layer of connective tissue that covers
the prostate). So, no further treatment required.
Normally assessed as complete cure after results
(probably PSA) clear after 5 years.
Impotence:
Not really tried getting erection at this early stage.
And, being widowed, I'm not to bothered. To me, the more
important issue is continence.
Dr Ta said that ultimately, I'd be eligible for Viagra, a
penis-ring and pump! But, we shall see if I bother.
Returning
to vigorous exercise:
At the earliest, he said 6 weeks, and even then, gently
ease back into it. My interest is cycling.
"Most of the internal tissues will have healed by
then, and gained their maximum strength."
"More leakage may occur" - as I suspected -
"because of the greater abdominal pressure".
But I could simply wear a more absorbant pad to start
with. We shall find out.
Also,
the Anti-embolism stockings: YES! He
said I could stop those now. (it's been just over 1 month
since my surgery)
Follow-up
PSA test at 3 months, then further consultation - at
present, it appears to be booked for Monday 29th June. I
might try to get that brought forward a bit.
31st
March 2020 - general
progress
So how's things progressing?
Well, all glues & stitches off, except one just above
naval, where the glue is mostly loose.
Continence: Much
improved! Needing inly one light pad at night, and
another in the day. ("Light" corresponds to the
3 drips symbol")
Doubtless mostly a result of my doing plently of Squeezy excersises. Now I do 5 per
day.
It's likely I will return to a reasonably good level of
continence in the next few weeks, and within a month may
need only one light pad per 24 hour period.
Managing more excersise: walking in excess of 3 miles per
day. Remember: at the time of writing this, all of UK is
in lockdown due to Covid-19. So this becomes my one
"rationed" walk per day!
I
will pause here, to give God thanks - that my surgery was
performed, my catheter removed, all before the Covid-19
UK lockdown.
I had
planned on returning to work yesterday (30th March), but
I'm effectively benefitting from a very extended period
of recouperation!
Only down side is I've been laid off work.
16th
March - my
continence
Encouraging. Only needed a nappy the day my catheter was
removed (12th March - see below). Wore one that night in
bed, but it was still dry in the morining!
Been
doing the Pelvic Floor excersises. The NHS App, 2.99GBP
when I bought it, is very handy, it does
help you keep track of the excersises. "Squeezy
For Men"
Obviously, on a mobile device, search on your apple store
or google play.
Today,
I'm trying to see if I can manage the day with just a
level 2 pad. Mostly, I leak slightly when I cough, stand
up or blow my nose. Not
leaking other than then, for which I'm thankful.
Hopefully, I'll be fully dry sometime in the months to
come.
Wounds
- glue starting to curl off some ot them. Today, one was
holding on only by one stitch - cut that with wire
cutters (my risk!); all ok, wound joined with no seeping.
14th
March So - because of my decreasing sodium
level, went for a walk and bought 2 jars of anchovies,
packets of hoola-hoops, and salted peanuts. (My normal
diet is to avoid uneccesary salt!)
"I spoke to Andrew over the phone today as we have
converted all our clinics to telephone calls due to
coronavirus.
Andrew had previous HIFU and cryotherapy for his prostate
cancer. He underwent a robotic prostatectomy on February
27 and I am pleased to report that he is doing very well.
His final histology revealed a Gleason 3+4 cancer, which
was organ confined and clear margins were achieved.
From a functional point of view, he is down to just two
small pads a day. He has some day time leakage with
coughing and sneezing, but is almost dry at night. I
expect this will continue to improve. Unfortunately he
has not yet had return of erectile function, but we will
continue to monitor this for now.
We will speak to him again in around 6-8 weeks time after
a PSA test. He may have this done locally if he cannot
get into UCLH easily."
12th
March 2020 Cystogram was very thourough -
performed at UCLH (been unable to find a better web link
to the details - please let me know if you do!).
I was
able to see the x-rays of my bladder on the screen.
They
were checking that the point at which the surgeon had
re-joined my urethra at the neck of my bladder had healed
well. During this time, the nurse needed to push the
catheter further into my bladder. When it was difficult,
she asked if I minded her pulling back my foreskin! Ok, a
bit of a fun thing to mention for you! I also advised her
to try lubricant, which also helped with pushing the
catheter in.
When they were eventually happy with the cystogram results, they removed my
catheter.
So I sat up on the x-ray bed, and immediately started to
leak!
I was given a nappy and a towel.
Then, spent a few hours in the canteen drinking coffee
and juice so I could prove I could void (pee) ok.
No problem there - was slowly leaking into the nappy
anyway!
Within a day or so, I only needed incontinence pads, not
nappies. Since locally sourced incontinence pads are a
bit expensive, I've taken the nurses advice and now use
Boots own brand. Started with the Normal, but see above for more
recent improvements.
27th
February 2020 Praise God! By Monday (24th)
lunchtime, I'd arraged my surgery for Thursday that week!
And again thankful! I was first on the list.
Recovery: very painful - ended up on a jab of Morphene
(lovely experience!)
Came home next day - most uncomfortable UBER ride over
the speed humps - the car was ok - but because of my
surgery, I felt every slight bump!!
Been impressed with how quickly the surgical skin wounds
from the robot stopped being significantly painful.
Now on the recovery route (as of 7th March)
Have
to give meself daily injections (ouch!). Pre-loaded
syringes of enoxaparin thromboprolaxis.
Cystogram
(to check for leakage where he's sewn my urethra back
together) and if ok removal of catheter: on Thursday 12th
March.
Will then see if I'm dry (continent) or not.
I
have had a relative staying with me this week and last,
so that's a great help. Been for a few short walks (about
500m) with them. Also just about managed to sit through a
1-hour piano concert on Saturday 7th March. Am using a
pressure relief ring cushion that helps greatly.
Planning
on going over the road to a local Church later this
morning (Sunday 8th March).
Catheter
experience: this is the 3rd catheter I've had to have,
must say is the most comfortable so far! Possibly
different catheter material?
Also, when I asked for a method of securing it at the top
of my thigh, they used a stabiliser.
Gave me much more confidence, particularly as this time
the catheter was in for 2 weeks.
21st
February 2020
Had consultation with Dr
Senthil Nathan. Told him I'd decided on his
surgical option.
Then saw Heather and hugged and thanked her
for her help in all this. Yes, It's quite an emotional
experience!
Dr Nathan said he'd requested a surgical appointment.
7th
February 2020
Started the day at 9am at Hallam Conference Centre 44
Hallam Street (just minutes from Great Portland St
London)
A good presentation by Surgeon
Greig Shaw
(Their "medical school").
Went through details of Radical Prostatectomy using the
Da Vinci Robotic machine. Also passed around a few of the
probes used in patients.
Allowed for interactive questions, of which I provided
quite a few!
Then a presentation from two clinical nurse specialists
who dealt with pracical issues such as catheter and the
injections they send you home with to use to prevent
blood clots.
Then onto my consultation with surgeon Dr
Senthil Nathan. Bit blown away with the details.
First time I've spoken to a radical surgeon for over 5
years!
Then to oncologist Heather for my (now) second
consultation. Because I was still undecided re Surgery or
Radiotherapy she said she wouldn't give me the first
hormone injection as originally intended. (It would have
made surgery more difficult if I chose that). Instead,
I'm continuing on the (milder) hormone tabs (Bicalutamide
50mg 1/daily) which are also halting any growth in my
cancer.
I'm seriously considering surgery now - but then, I seem
to change my mind every two days! Good reason indeed, for
me to make this a matter of prayer. Surgery does sound
far more elegant than the grueling hormone &
radiotherapy route, with it's possible permanent bowel
and/or rectal issues.
But I am very fit, which I figure will be a bonus for
recovery and return of continence if I choose surgery.
Because I've already had HIFU, I'm kind-of resigned to
being impotent after either treatment I have. But we will
have to wait and see.
I have a surgeon consultation this Friday 21st February
in the morning then with Heather in the afternoon. I'm
preparing questions for each of them to try to clarify
things before my decision.
Will update this blog soon, and include my final decision
of this coming Friday 21st.
The
focal therapy is over. Now begins hormone and
radiotherapy.
My
hope that my apparently-decreasing PSA (see below) over
recent months, would mean we could
"watchful-wait" and "hope" the cancer
might go away: she said that "the biopsy trumps the
MRI".
- see below, 7th January. This is what I expected to be
likely.
Hence, the cancer does need treating, and the only
options at UCLH now are 1. Radical Prostatectomy
(surgery), 2. Radiotherapy
She confirmed the general medical consensus, that Radiotherapy appears to result in less
likelyhood of lasting problems afterwards, than does
radical prostatectomy.
I'd already made up my mind that I'd prefer radiotherapy.
The downside is that it's several months of treatment and
side-effects, whereas surgerty is over in one day,
although recovery can take weeks.
Result:
Hormone
Therapy
has started now: Heather prescribed me hormone tablets
Bicalutamide 50mg 1/daily.
I'll then return next Friday (7th February) for my first
hormone injection.
I
told Heather, again, of my dissapointment that hormone
therapy won't make me into a soprano (I sing bass at the
moment) (!)
Radiotherapy to start July.
Heather agreed that I've managed to postpone this moment
for 6 years with focal therapy.
But
she would still like me (and I'd also like) to understand
a bit more about surgery.
So my very busy Friday 7th February will have this
programme:
8:45am
group presntation about surgery
12:20am discussion with a surgeon
13:30 first hormone injection with Heather
As I
see it, I could still change my mind and have Radical
Prostatectomy right up to the time before my Radiotherapy
starts probably in July 2020.
Summary
of PSA over recent months
My readings to date:
9 Nov 2018
14
May
2019
21 June
2019
Sept 2019
4 Dec
2019
5.2
HIFU
5.9
5.3
4.8
20th January
I told my MD how God's timing had worked out the timing
of the previous three days, 15th - 17th January!
I told her about the likely treatment, how it may involve
the 2 hours each working day, during the later 7-8 weeks.
She then spoke to my boss and the workload planner to
summarise how it would affect my working hours.
Basically, it will probably involve 2 hours off work for
the 7.5 weeks.
But that's why I chose the UCLH hospital all those 6
years ago - it's conveniently near to my office
17th
January 2020
Consultation with Prof
Heather Payne
Was told that radical prostatectomy was probably not
ideal, because of the small prostate.
Radiotherapy probably best treatment.
Given details of it - I was told it'd be around 10 months
hormone
therapy,
with the radiotherapy starting around 3 months in. The
hormone treatment involves only a montly
injection/implantation of a pellet, pobably done at my GP
clinic.
For details of the radiotherapy click
here.
I asked abou the Proton Beam Therapy - a new centre
opening there later this year.
I was told there's no advantage in protons over
radiotherapy for prostate treatment.
Brachytherapy - they do only whole
gland, and that needs a solid
prostate, which I don't have, after having had 2 lots of
focla therapy.
Heather said her team would discuss me at their next
Friday meeting (24th January), when they meet with my
previous focal team to discuss patients.
16th
January 2020 How God overrules!
When I told my company the not-so-good news, both the MD
and CEO called me in to his office.
They expressed concern, and offered to help in any way
they could.
15th
January 2020
Consultation - very pleased that I was seen by Prof Mark
Emberton!
But news not good; but honestly probably what I
suspected.
I have low-to-mid grace cancer in the right hand side,
(enhanced area) gleeson 3+4, 6mm. Left hand side
(previously treated area) is clear.
See my latest
MRI scan.
"No further focal therapy is possible. My prostate
is now tiny. The cancer is too near the sphincter."
"You're making new cancers."
Well, I am an electronics design engineer, but didn't
realise that at the same time, I was making new cancers
also!
He referred me to the radiotherapy team. Appointment
arranged to see Prof
Heather Payne on Friday 17th.
10th
January 2020
PET Scan at UCLH
Nuclear Medicine
Very well organised: was called in slightly before
appointment time.
[18F]PSMA-1007 injection, 1 hour wait in the small
cubicle
(I joked on Whatsapp how it was like being confined to a
cell 'cos I was radioactive!), then a bit over 1 hour
later the scan.
Lovely new
scanner
Took two diazipam sedatives (GP prescribed) because I'm
calustrophobic.
Most uncomfortable part was having my arms above my head
throughout the scan - see the straps at the grey headrest
on the table.
Follow-up
appointment on Wednesday 15th January.
7th
January 2020 Template Biopsy at UCLH
Cancer Centre
Dr Thomas Collins said he'd be sampling more than just
the enhanced
area.
Went very well: arrived prompt for 7.30am. was in theatre
a bit before 9am.
During recovery, more comfortable than after previous
biopsy.
My
observation: my PSA seems to have
slowly decreased over 6 months: 5.9, 5.3, 4.8 (see
below). So, it could simply be that it's doing so slowly.
This may be one indicator that there isn't significant
cancer still in my prostate.The biopsy above will show
more precise detail.
4th
December 2019 Consultatioin with Caroline
Moore
Summary:
My MRI of 6th November "has shown some enhancement
on the right side of the prostate"
For further details of this consultation including MRI
image
PSA test returned 4.8
Template biopsy now booked for Tuesday 7th January 2019
Wholebody
PET scan booked for 10th January 2019
27th
September 2019 PSA test returned 5.3.
Emailed the UCLH Prostate Cancer Clinic Nurses, told them
Dr Thomas had previously said they'd probably re-MRI if
my 5.9 PSA figure hadn't dropped below 4 by Semptember.
They said they'd review me at their Weekly Monday
Meeting.
I then had an MRI at UCLH on 6th November.
I now have a follow-up appointment arrnaged for the
morning of December 4th at UCLH, Westmoorland Street.
19th
July 2019
See link below for more explicit details of my progress,
including Dr Thomas' consultation letter.
10th
July 2019 MSU result
normal. Consultation
at UCLH
Seen by Dr Thomas Collins.
He wasn't surprised by my increased PSA (see below).
I'll ask my GP for another PSA test in September. If the
result is not lower, then I'll try emailing UCLH to see
if they'll give me an earlier consultation than the one
he arranged for June next year.
I'll get a separate appointment for an MRI in May 2020.
It's possible I may be given an earlier one if my next
PSA level hasn't decreased.
Since
I haven't had any recurrence of cancer in my RHS that was
treated, I asked him if it's equally likely I won't get a
recurrence in my LHS. His comment was that "there's
a 1 in 4 chance of it recurring after treatment".
5th
July 2019 MSU sample provided.
No results as of 9th July.
Hopefully will have before my consultaion tomorrow,
although I don't think it'll influence what the surgeon
says much.
21st
June 2019 PSA blood test done; result 5.9
This is up from my November 2018 figure of 5.2
A week later, GP refused a re-test within less than 3
months - "It won't have changed yet".
But they did agree to an MSU (MId- Stream Urine) test
I
queried this with UCLH hospital.
The Clinical Nurse Specialits emailed me back:
"The PSA can still be high at 3 months post HIFU due
to some swelling of the prostate. We usually just check
again at 6 months and if not down then would consider an
MRI at that point. I think an MSU is a good idea
It's always best not to cycle or have any sexual activity
for 2-3 days before a PSA test also" (First time I'd
heard that!)
4th
June 2019 Retention re-test: now only 82ml !
Praise God for that! The threshold figure is 100ml.
Good that my anxieties about needing a lifelong catheter
are no more!
24
May 2019 Finding voiding sometimes a little
painful.
I contacted the Clinical Nurse Specialists by email
(supplied in their info booklet on discharge) and asked
about it:
"Is it normal to sometimes experience a little
urethral pain when voiding?"
"Yes it is on and off for 6 weeks. If there is a lot
or the urine is smelly take a sample to the GP for them
to test"
21st
May 2019
At trial without catheter (TWOC) clinic.
Catheter removed, pretty-well painless.
Then: around 3 hours of recording drinking and voiding
(pee-ing)!
Voided volumes good, but retention (post-void residual,
PVR) measured at around 170ml, which is a bit high. No
better after voiding 30 minutes later.
Discussed
with nurse, and arranged an informal (no appointment
required) re-visit to her at TWOC clinic in 2 weeks time
(4th June) to re-check PVR. "Just knock on the door
at about 11am".
She said HIFU does cause the prostate to inflame
initially more that cryo; in earlier years, some patients
were re-cathetered, but not now.
Concern is too much retention could cause bladder
infection.
Hopefully, retention will decrease to an acceptable level
(around 100ml) within the next 2 weeks. It'd be tedious
to have to take lifelong medication, and I don't relish
the idea of another catheter.
Additional
observation: I've been passing a small fragment
(presumably of my ablated area) each time I void.
14th
May 2019
Had HIFU at UCLH
Cancer Centre
Was seen farly promptly after my 7:30 admission; whole
procedure was finished just before 11am, after which time
I was in recovery then settling in the ward.
Before the procedue, I asked the surgeon to ablate only
as much as necessary. She said she'd try to leave the
very left side (near my prostate edge) not ablated.
Most uncomfortable part is now at home, with a urethral
catheter for 7 days.
Time will tell how effective the HIFU has been, both from
a follow-up MRI (in 1 year's time), 3- monthly PSA tests,
and also over the months as to continence and erectile
issues.
Catheter due out on Tuesday 21st May.
I
enquired via email to a UCLH Uro-Oncology Nurse
Specialist as to why I wouldn't have an MRI a few weeks
after my HIFU, like I did 5 years ago after my Cryo.
(Scroll down a bit to see those MRI scans and the one
titled "18 days after cryotherapy").
I was concerned the ablated area would not be visible in
1 year's time.
They told me: "We don’t
routinely do MRI after HIFU like we do after cryotherapy
, we can still see the ablated area after 1 year".
Now,
I assume that either the ablated area won't shrink or
that their definintion of we can
still see the ablated area after 1 year really
means the "black hole" will be visible or only
scar tissue, remains to be seen.
Next
appointment after my catheter removal: 10th July in
clinic for, presumably, a review. I've booked a PSA test
at my GP's for Friday 21st June.
20th
March 2019 Consultation with Prof
Caroline Moore, at Westmoreland Street:
Cancer confirmed at the two points that were highlighted
on the MRI.
I have 5mm posterior of gleason 3+4, 3mm anterior of
gleason 3+4. Click
here to
see the now annotated diagrams. Click
here to
see the histopathology report.
The
way forward: I was given the option
of radical prostatectomy, radiation or HIFU. I would like
to retain my prostate for as long as possible, so I've
chosen to have HIFU. Waiting confirmation of surgery
date.
I asked about Cryotherapy again; I was told, as I
suspected, that Cryo could not be done in the posterior
area, since it's too close to my rectum.
Caroline did mention that if I didsubsequently need a radical prostatectomy, it
may be more difficult to ensure no cancer remained
outside of my prostate. However, HIFU is the route I've
chosen.
I'm
also hoping that this HIFU may mean I won't ever develop
significant prostate cancer again, although I accept that
this cannot be guaranteed.
Caroline said that I would have a left hemi-ablation, in
other words (I assume) the left of my porstate will be
destroyed. This should destroy both my anterior 3mm and
the posterior 5mm cancer.
Click
HERE for explanation of HIFU
Click HERE for my now annotated MIRI
report.
Friday
22nd February 2019: Template Bipopsy
performed by Dr
Thomas Collins on the NHS at McMillan
Cancer Centre
This is a really nice, fairly new building.
I was told after recovery that 8 samples were taken (this
requires verification at the follow-up consultation, I
might have heard wrong in the ward).
This is much less than in 2013, where 24
samples were taken. On that occasion, there was a
clearly defined, very likely tumour visible on the MRI.
But this year (2019), I assume only 8 were taken because
there was not a very likely tumour visible on the MRI.
Sedation:
Before my biopsy, I was concerned when I was told by the
anaesthetist that I would not be having a general
anaesthetic, but instead deep sedation. I was worried I'd
be aware of what was going on during the biopsies.
I needn't have worried: I was "out" just as if
I'd had a genereal anaesthetic. As with a general
anaesthetic, the next thing I knew, I was waking up in
recovery.
The main difference is that you breath yourself, and
don't require ventilation as with a general anaesthetic.
This deep sedation is probably more suitable for very
short procedures such as this biopsy.
Another interesting detail is that, when I told the
anaethetist I vomited after my last general anaesthetic
(a common recovery effect), he said he'd give me
anti-nausea medication as part of my wake-up drugs.
Now
waiting for follow-up consultation appointment.
Update
February 2019
Because of forecast of heavy snow, managed to re-arrange
UCLH consultation for 1st February as a phone
consultation at the same date & time. Apparently they
do that often - many of their patients live far away.
The consultant, Clement
Orczyk,
Said he would request a Template Biopsy for me. I
subsequently had a pre-assessment on 6th February.
Update
5 December 2018 MRI results are indicative of possibly
significant cancer, but will only be sure if I have a
biopsy. Professor Caroline Moore at Londn Urology
Associates has written to my GP, asking him to refer me
back to her team at UCLH NHS hospital for a Template
Biopsy.
She did say we could monitor my PSA on a 4-monthly
frequency, but because the pattern of steady increase in
PSA is in keeping with that leading up to my previous
diagnosis, I've elected for a biopsy.
Also, regarding the supposedly higer PSA value threshold
for someone my age (65), Caroline said that does not
apply to someone like me, who has
had prostate cancer before.
For a
full report from the Medical Imaging team, click here. This will open a new
browser window.
Update
9th November 2018 - PSA 5.2ug/L
GP said to re-test in January, since for my age, 65, the
threshold is supposedly 5.0, not 4.
However, I expressed concern that the steady increase
over the past few years is in keeping with the values I
had leading up to my diagnosis in 2013. Hence he agreed
to refer me back to the urology team. I've chosen to
start, as I did in 2013/2014, with the private clinic at Harley Street. My insurance will fully
cover the consultations and MRI (if I have one). If I
need further tests/treatment that they will only do at
Princess Grace Hospital, then because that hospital isn't
covered by my insurers, I'll probably ask to be referred
back to the team on the NHS, at UCLH.
COMPARISON OF PSA TREND
POST-PROCEDURE, WITH with PRE-PROCEDURE TREND
Procedure date: 21st April 2014
My Post-Procedure readings to date:
May 2015
Jan 2016
June 2016
Feb 2017
Oct 2017
Dec 1017
Nov 2018
2.54
3.22
3.7
3.6
4.5
4.0
5.2
My readings prior to my procedure in 2014:
2009
2011
Mar 2012
Jan 2013
June 2013
Jan 2014
2.61
3.94
4.19
4.93
6.2
5.8
IMPORTANT!
This
TREND in PSA readings is the IMPORTANT thing to monitor.
A SINGLE PSA READING is not sufficient, it can be
unreliable.
I've
a consultation appointment at Harley Street on Monday 3rd
December.
Update
4th December 2017 - PSA 4.0ug/L This
is considered as "normal" on my GP report,
"no action needed". My conclusion: although
it's good that I don't need to take any action, the trend
over the last 2 years is upwards. It may be that this
will be the last time it will be 4.0ug/L or less. We will
see.
Update
13th October 2017 - PSA 4.5ug/L This
is slightly above the ideal threshold of 4.0. However,
based my "Hospital consultation at UCLH" about 1 year
ago, (see below) and chatting to my GP, I'll have a
repeat PSA in a few months time. And soon I'll provide a Mid-Stream-Urine specimen.
Update
February 2017: PSA 3.6ug/L. This
indicates that the cryotherapy is remaining effective -
the cancer tumour appears to have been effectively
destroyed, with no evidence of recurrence.
Update
June 2016: PSA 3.7 ug/L
Update
January 2016: PSA 3.22ug/l. Prostate
volume 23cc
Hospital consultation at UCLH Westmoreland Street (This is
the new loacation of the Urology department. It is no
longer in the Cancer Centre in Huntley Street.) : My cancer is now stable,
no evidence of any significant prostate cancer,
Recommendation: Remote Surveillance. Get 6 monthly PSA
test done at my GP. If it goes above 4, then also do
Mid-Stream-Urine test, to check for an infection that may
be giving the higher reading. No need for another MRI
provided PSA remains below 4, see above.
[My understanding]: Repeat PSA 3 months later. If still
above 4, then go back to the hospital for advice. Note: a 6 monthly PSA test should be
mandatory for everyman aged 50+, see my notes at the
beginning of this blog.
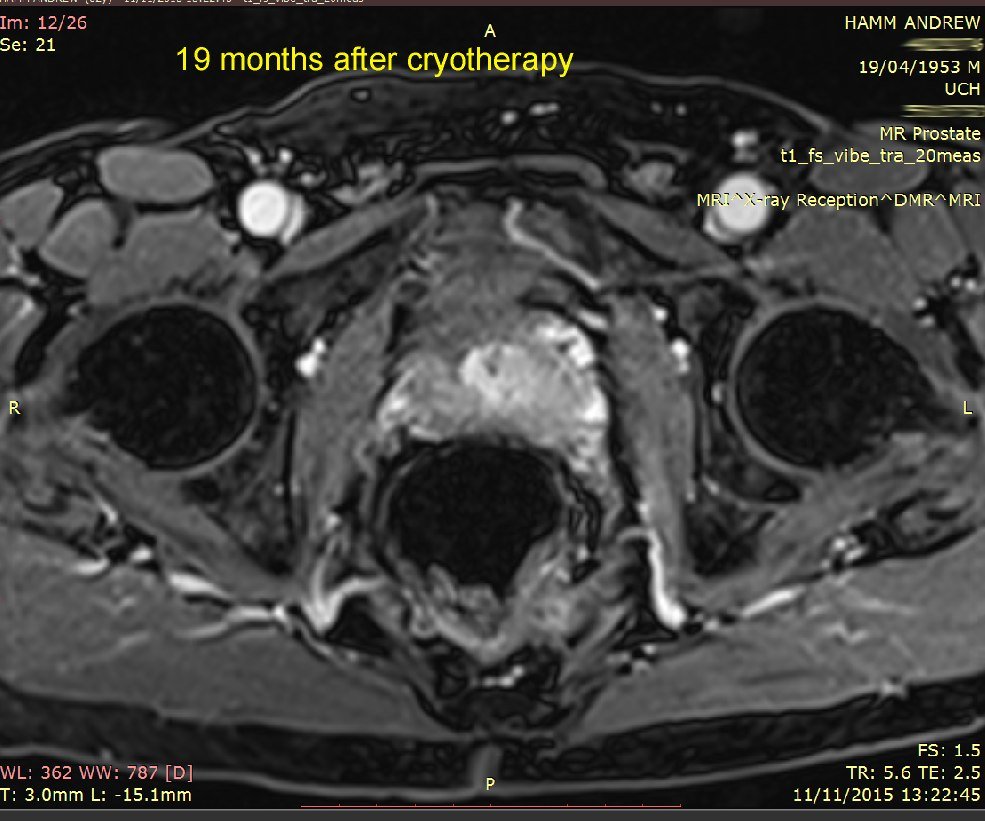
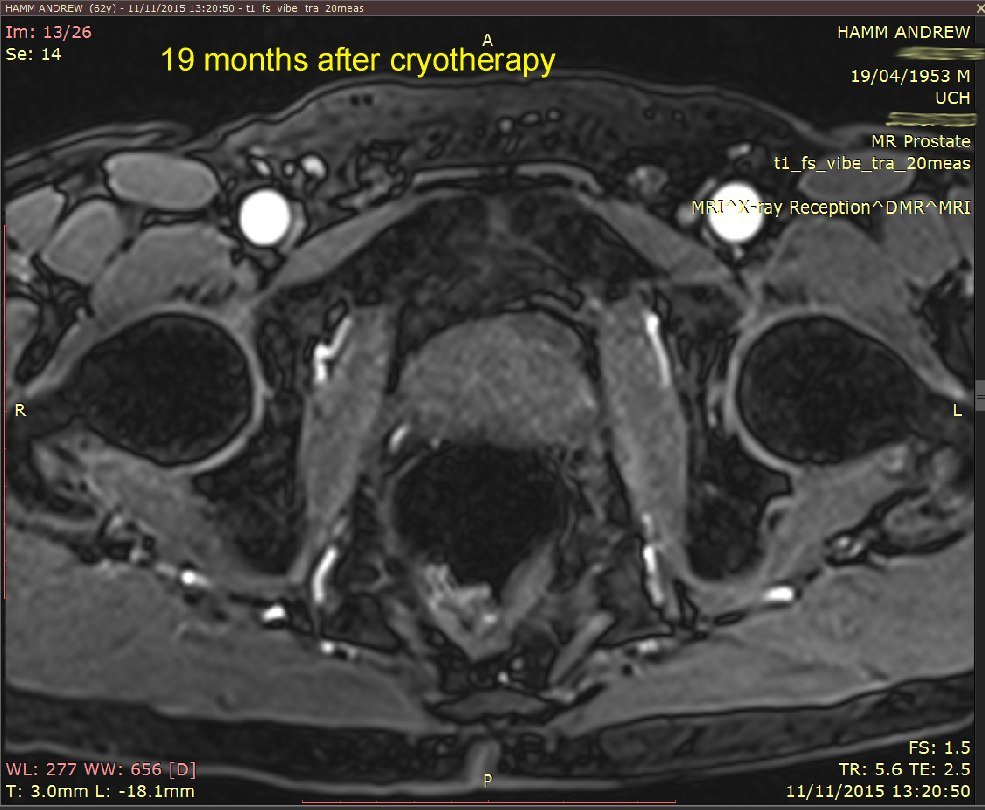
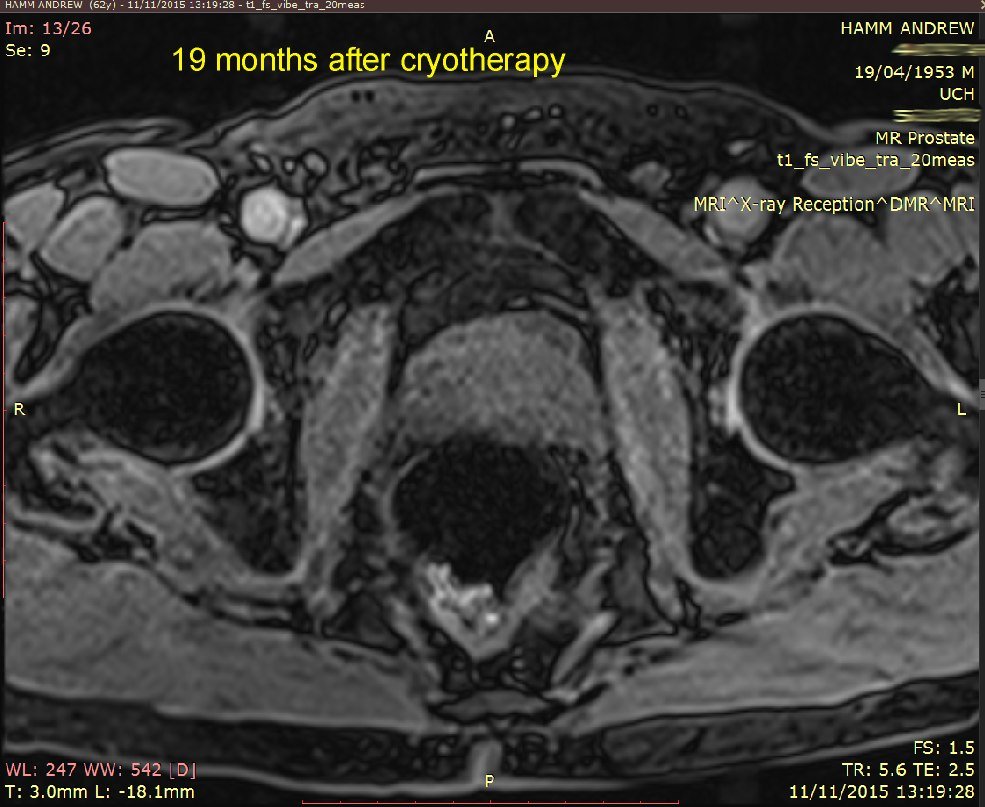
I've put 3 MRI images taken in November 2015. Compare
these with my earlier ones below that, from 24 November
2014. Whilst not commenting specifically on these, the
consultant said that the overall MRI had not revealed any
significant (observable) prostate cancer.
[My observation]: I'm at no more
risk from prostate cancer than any other man my age.
PSA result, May 2015: 2.54. This is
a slight reduction from 3.1 measured in November 2014.
So, it's a trend in the right direction.
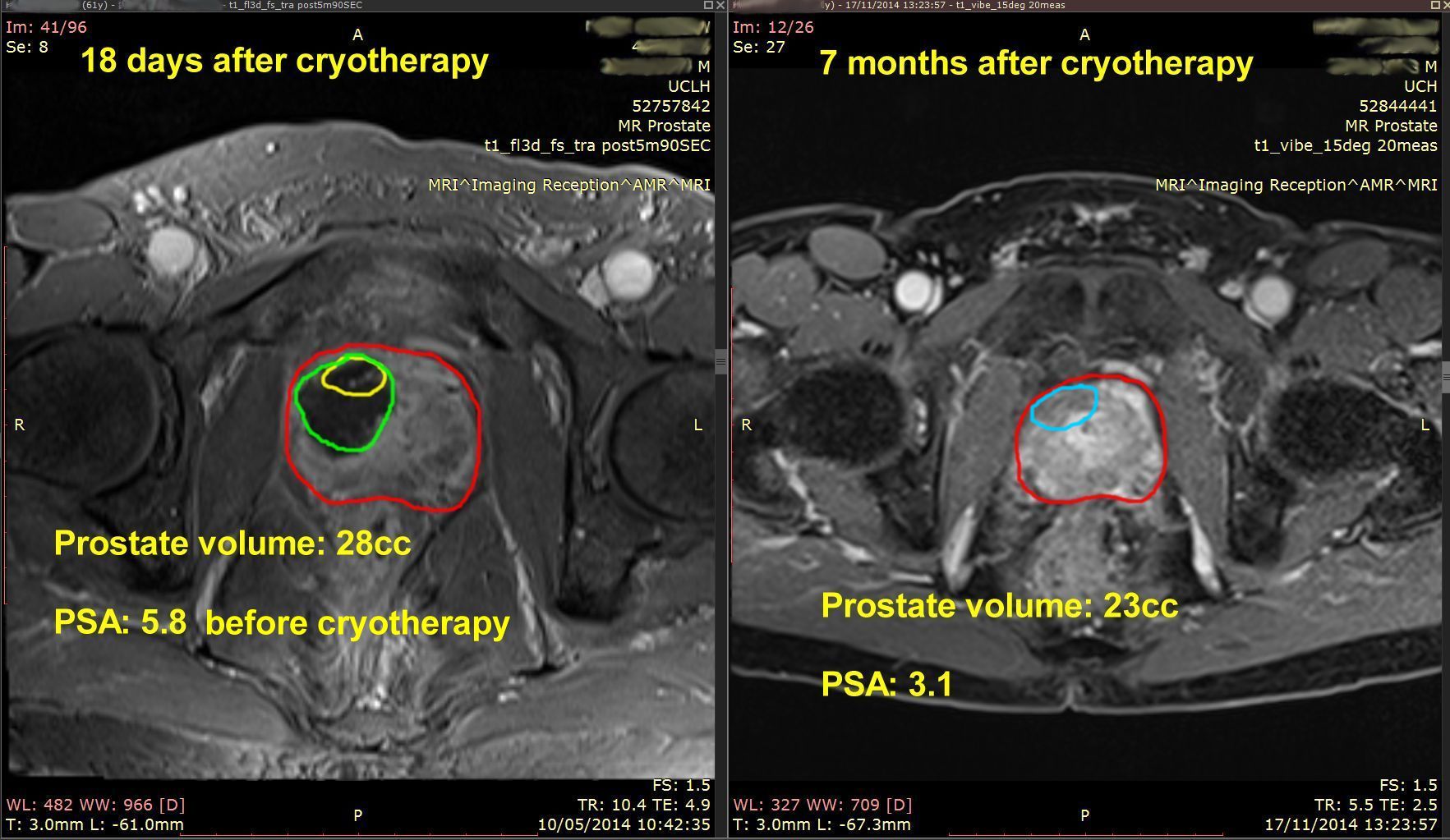
[the
following notes added on 24 November 2014]
18-day and 7-month MRI and PSA comparison - see image
below.
Explanation:
my prostate is roughly outlined in RED.
The original location of the tumour is roughly outlined
in YELLOW on the 18-days image.
The ablated area is outlined in GREEN on the 18-days
image.
These
results show:
The
ablated area has shrunk to (I presume) no volume at all.
My prostate volume has reduced by 5cc, which is pretty
close to the 5cc volume that Emberton estimated would be
ablated.
My PSA has rougly HALVED. The present PSA of 3.1 is
within the range expected for a man of my age (61 years)
who does not have significant prostate cancer.
My
conclusion: Success! Cancer treated*.
Side effect: reduced ejaculation.
Future plan for tests, surveillance: to be discussed on
10th December with Emberton.
Watch this space! better still, check
my latest results.
*The
significant anterior tumour has been treated. I am not
experienced enough to recognise any remaining lower-grade
cancer by looking at the MRI image.
Update
10th December 2014: Had follow-up
consultation with Emberton.
He said that it was "all good!" See
below for his dictated letter which gives a precise
statement of his observations.
He
said that there was scar tissue, outlined in the 2nd
image above in BLUE. I guess this is the left-over bit of
the ablated area, see the 1st image above, outlined in
GREEN.
He
did not make any comments about any further cancer being
visible, probably because my PSA now of about 3 does not
suggest there IS any significant cancer. Remember: all
men my age will have some very low-grade prostate cancer,
but it will probably never grow fast enough to catch up
with them as they age.
There is even talk of not
considering low grade prostate
cancer as cancer, see this
link.
The
future: I am to organise 6-monthly PSA tests throgh my
GP. If my PSA goes above 4, then I am to contact Emberton
again.
He
has arranged another MRI scan for me in 1 years' time
(November 2015).
Note
that the 6-monthly PSA tests are what I was having for
several years before my
diagnosis of cancer.
As I say at the beginning of this blog, it's very
advisable for all men
over 50 years old, to start having 6-montly PSA tests and
continue them for the rest of their lives.
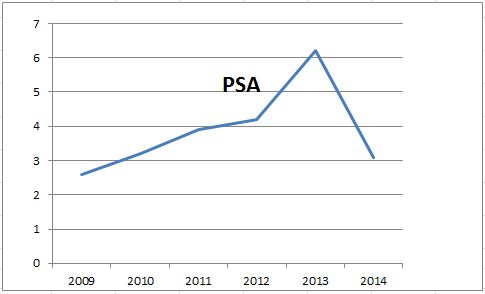
A
graph of my PSA is shown below. (The best graph I could
make; my PSA probably dropped much faster than the slope
shows, from a figure of about 6 before my cryotherapy, to
a figure of about 3, soon after my cryotherapy that I had
in April 2014).
My
PSA steadily climbed over the years, until it reached
about 6.
Then, the cryotherapy knocked it down to about 3 again.
If it climbes again above 4, then I'll have further
tests. If necessary, repeat treatment will be given.
However, it may well be that any remaining low-grade
cancer will never develop in my lifetime to cause any
trouble, see this
link.
This
report above is the very latest update to this blog.
Apologies again for it all being a bit disjointed! I'll
get round to re-writing the whole page someday!
Update
February 2015: Regarding "...a
change in the quality of the ejaculate" mentioned
above: as mentioned elsewhere, my ejaculation diminished
to zero about 4 months after my cryotherapy. However, a
very little ejaculate does appear after orgasm.
Emberton is probably familiar with this process in some
patients, hence he would classify this as "diminished
ejaculaion", and not "zero".
My erections and sexual desire remain good and unaltered.
Update January 2015:
Just received my copy of Emberton's consultation letter.
"....he
has done fantastically well with almost no toxicity. The
only thing he has noticed is a change in the quality of
the ejaculate, which we would expect, treating in the
anterior component. His PSA is now steady at 3.1 mcg/L
and the MRI shows no residual disease on the
late [24 November 2014] scan. We would recommend PSA's
on a six monthly basis and look forward to seeing him in
December 2015, with an MRI beforehand."
Post-surgery
(and post MRI) consultation on 28 May 2014
Surgeon had already
said the post-surgery MRI
(one picture I sent him) looked good. This was an
initial MRI
scan, only 2½ weeks after my surgery. The one in
November will give a better idea of the status of
any remaining cancer.
Since
then, he'd had an opportunity to look at the
whole set of post-surgery MRI images.
He said that these preliminary images suggested
that the significant cancer had been destroyed
(ablated).
Unlike
Prof. Emberton, he couldn't bring up my MRI
images on his consulting room computer.
So: before my next MRI, need to see if I can find
a DICOM viewer for Android.....(!)
[13 June 2014]: found
a DICOM app for android! "Simply DICOM"
it's called. Can see clearly the ablated area.
Wish I'd had this for my consultation 3 weeks
ago! I'd have been ahead of the surgeon!
So from now on, we can discuss my MRI pics using
my phone!
The
ablated area is the dark area.
He
also said that it was originally
significant, and did not fit into the category of
being able to be left untreated for surveillance.
"Anyone",
he said (meaning "any" urologist),
"would have taken action". This is
because the maximum cancer core length was 12mm,
a significant size.
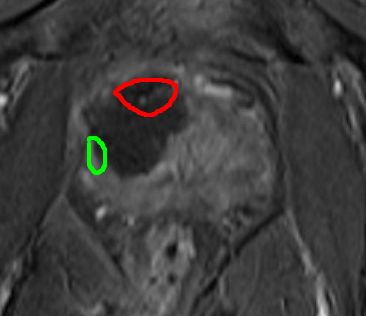
The
ablated area extended significantly below where
the anterior tumour had been (see annotated
sketch - original tumour outlined in red).
Commenting
on this, he said:
"The ice-ball (produced by the cryotherapy)
would have done that". Basically, that's the
best precision that could be achieved. But an
advantage may be that it may have also partially
destroyed the peripheral 3 + 3 cancer on the
right hand side, (marked as a green area). Even
though I had asked him not to,
the cryo could not be controlled precisely enough
not to destroy that.
I must admit I was in two minds as to whether I
should have asked him not to
destroy that 3 + 3 also; well, maybe it's happened
now!
My
second post - op MRI scan and first post-op PSA
blood test to be done in November.
Regarding
slight leakage when "busting" for the
loo: he said that should improve with time.
The
surgeon said that I am now
over the main, initial recovery period.
To
see the Webcast where Prof Emberton answers
viewers questions, click
here.
Then, search for "Live interview with
Professor Emberton"
NanoKnife is mentioned in the video at the 19
minutes slider position.
You need to be referred by your GP.
Under the Patient Choice option, you can ask to
be referred there even if you do not live in the
central London Area.
This is your right,click here
to see my referral letter.
Recently
changed:
Upper Ground
Floor, Outpatients,
University College Hospital at
Westmoreland Street
16 - 18 Westmoreland Street
London W1G 8PH
Nisma Akhtar is PA for Emberton and
his team:
Telephone 020 3447 9194
or 020 3447 9485 (main dept)
Emberton and
Caroline Moore's Private referral address - click on the link
on the right
Note:
if you're thinking of having private treatment
under Emberton, check that your insurance covers
the imaging
place and
the hospital that Emberton uses.
I opted out of private treatment after my TPM
Biopsy, and had my final cryo done on the NHS, as
I explain above.
Also,
for a private consultation with Emberton, you don't
have to be referred by your GP (as you do for NHS UCLH).
If you are self-funding, you can simply go along
and refer yourself.
Otherwise, check with your insurance first.
Not
sure how to interpret this BBC article! Perhaps
it reflects the fact that many men still aren't
benefitting from the greater accuracy of the MRI
& TPM Biopsy test, or that even that
can't predict how aggressive the cancer is.
I admit that it appears uncertain how quickly my
anterior tumour would grow, if it were left
alone. But see consultation above.
Pity it doesn't even mention
focal therapy!
Focal therapy is an amazing
treatment.
However, it can still only cure my body until it will die
anyway. But praise
God: I'm assured of eternal
life because I believe in the
atoning work done by Jesus Christ, when he died for my
sin, and rose again! You
too can have this same eternal
assurance, if you believe!